Youth Climate Health Solutions in Tanzania
Matama District, Tanzania
Amplify Health and Development in Africa (AHDA)
Climate change is intensifying health risks in Tanzania’s coastal districts, where communities depend on rain-fed agriculture and limited health infrastructure. In Mtama District, Lindi Region, rising temperatures, erratic rainfall, floods, and prolonged dry spells are undermining access to essential health services, food security, and psychosocial stability. Women, adolescent girls, and young people face heightened risks due to disrupted SRHR services, reduced household income, and increased caregiving burdens.
Youth and Community Health Workers (CHWs) are widely trusted and embedded within communities, yet remain underutilised in formal climate adaptation planning.

Research Methodology

Component
Design
Sample
Location
Timeline
Funding
Details
Mixed methods (quantitative survey + qualitative FGDs)
Mtama District, Lindi Region, Tanzania
Notes

208 survey respondents; 7 focus group discussions
Coastal district with high climate exposure
$10,000 (PERCC/Population Council award)
Part of PERCC case study porfolio

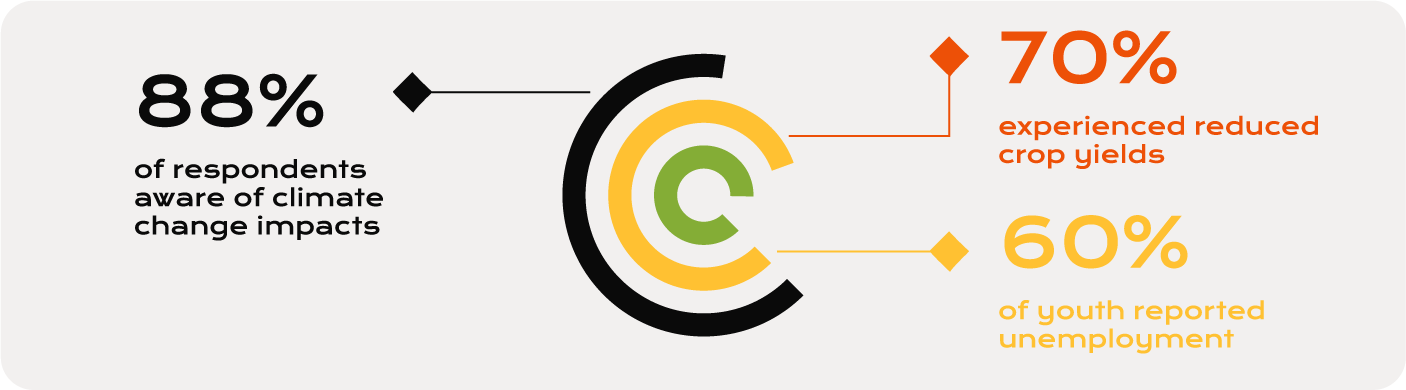
Key Findings
Extreme multi-hazard exposure: All households reported cyclone exposure (100%); 99% experienced salinity intrusion; 87% riverbank erosion. Over 70% rated impacts as high to catastrophic, citing livelihood loss, property damage, and water insecurity.
Pervasive mental health burden: Residents reported PTSD symptoms, anxiety, depression, and insomnia linked to past cyclones (Aila 2009, Amphan 2020). Environmental cues like strong winds trigger renewed panic. Livelihood collapse drives shame, despair, and social withdrawal, particularly among men.
Gendered and age-specific impacts: Women and adolescent girls experience compounded distress from unsafe water collection, reproductive health stigma linked to salinity, and caregiving burdens. Children show fear, behavioural changes, and school dropout.
Near-absence of formal mental health services: Only 1.8% sought professional mental health care. No formal MHPSS services exist at the union level. Mental health is absent from disaster planning, shelters, and primary care.
Strong informal coping, but insufficient: 93.6% relied on family support; 82.6% on faith-based practices. Community mobilisation (embankment reinforcement, coordinated evacuation) provides resilience but cannot replace structured services.
“The climate crisis in coastal Bangladesh is not only an environmental and economic disaster—it is a psychosocial disaster. Without addressing the mental health burden, resilience will remain out of reach.”
-Adapted from study findings, Gabura Union
Recommendations
1
Institutionalise youth and CHWs in district climate-health governance with defined roles, training, and operational funding.
2
Strengthen climate-resilient SRHR and mental health services through service continuity plans and integration of psychosocial support into primary healthcare.
3
Enhance community climate-health literacy and early warning systems through locally tailored education via schools, CHWs, and youth groups.
4
Improve multisectoral coordination and financing at district level by aligning health, agriculture, water, and environment plans and budgets.